After years of study and strong public support, the federal Office of Management and Budget finalized updates to federal standards for collecting race and ethnicity data, known as Statistical Policy Directive No. 15 (SPD 15).
SPD 15 is perhaps the most important federal policy supporting demographic data collection, as federal agencies must align their data collection policies according to its specified language, instructions, and measures. Alignment to SPD 15 is intended to result in more accurate and useful data on differences in population data based on race and ethnicity. The resulting data informs economic policy, health policy, housing policy, voting rights, civil rights enforcement, and other critical functions of government. In the health policy sphere, this change will affect everything from health research to quality measurement to culturally competent care and more.
Most importantly, changes to SPD 15 will greatly advance our understanding of the experiences of underserved and undercounted demographic populations, particularly those identifying as Latine and Middle Eastern/North African (MENA), by making them more visible in data. In health care programs, greater specificity in the data will result in more usable data on health care access, outcomes, differences, and disparities; help plan for and allocate resources for more culturally and linguistically competent care; and allow more targeted civil rights enforcement.
Major updates brought about by this change in policy include:
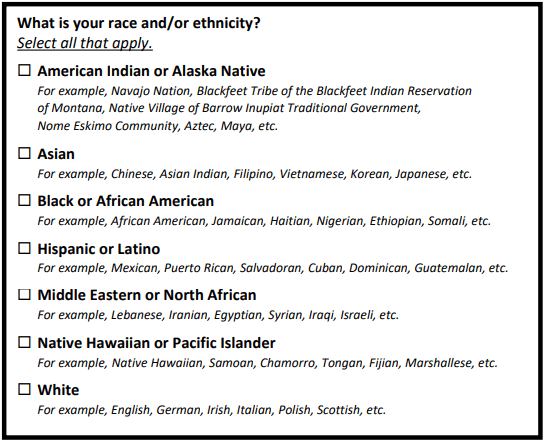
- Adding a new category – MENA – to the minimum set of race and ethnicity categories (current categories are American Indian/Alaska Native, Black or African American, Asian, Native Hawaiian or Pacific Islander, White, and Hispanic or Latino, see Measure 1, below). MENA advocates have asked for years – since the last update to SPD 15 was made in 1997 – to be included as a separate category. Now, MENA individuals have the opportunity to be directly counted in every federal data instrument, survey, and form.
- Asking race and ethnicity in one combined question. Although advocates are rightly concerned that race and ethnicity should not be conflated, testing reveals that respondents are more likely to choose a distinct option when given a combined question. When more people respond with a specific answer, as opposed to “other” or “multiracial,” more relevant, usable data on specific populations becomes available.
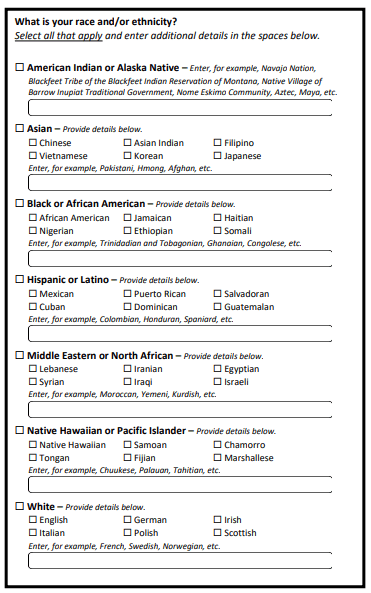
- Requiring use of a more detailed measure by default (see Measure 2, below). Wider use of the more detailed measure will help agencies gather enough information on smaller populations, such as Laotians or Salvadorians, to draw meaningful conclusions from the data. Agencies that want to use a less detailed version of the question (see Measure 1, below) will be required to request an exemption from OMB.
Measure 1
Measure 2
Agencies will be expected to begin updating their forms and data collection instruments immediately with a deadline of full compliance by 2029. While 2029 seems far off, many health insurance enrollment forms, published by the Centers for Medicare and Medicaid Services (CMS), are renewed yearly, and thus should be updated by the end of 2025. For example, forms that require yearly renewals include the Health Insurance Marketplace Single Streamlined Application and the Medicare Advantage and Prescription Drug Plan Enrollment Form, which both collect information on enrollee’s race and ethnicity. For existing data collection instruments that do not require yearly renewals, such as the T-MSIS system, which stores Medicaid enrollment and claims data from states, CMS will be expected to produce an action plan within 18 months, or about September 2025, that indicates when those instruments will be updated. Given that states use the T-MSIS system to report race and ethnicity of Medicaid and CHIP enrollees, CMS must work with states to come into compliance with SPD 15 within the expected time frame as well.
This change is encouraging—and long-awaited—and the federal government must continue this work to ensure that demographic data effectively addresses issues of systemic inequality. Along with implementing these changes to race and ethnicity measures, federal, state, and local governments must implement systems that routinely use data to study differences in health care access and address disparities. The Department of Health and Human Services must work diligently to adopt Sexual Orientation, Gender Identity, and Sex Characteristics (SOGISC) measures across health programs as written in its SOGI Data Action Plans. Similar work should occur to promote adoption of existing disability demographic measures and appropriate updates in line with the recommendations of disability advocates, researchers, and communities. Demographic data collection is just the beginning of the process, but it is a foundation that can drive equity for many years to come.